Blog
Trending Orthopedic Articles From Comprehensive Orthopaedics, S.C.

Should I Use Ice or Heat for My Aches and Pains?
Both hot and cold therapy can relieve pain and stiffness. But which one is right for you? Whether it’s during an intense...
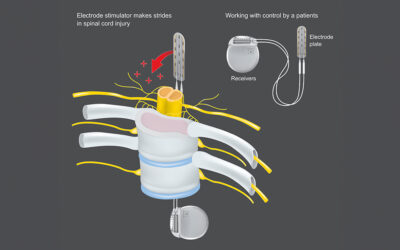
Spinal Cord Stimulation Eases Pain, Boosts Function for People With Prosthetic Legs
People who've lost a leg due to injury or disease are often plagued by what's known as phantom limb pain -- discomfort...

Arthritic Hands: What Works (and Doesn’t) to Ease the Pain?
Millions of people who live with the pain and stiffness of arthritis in their hands get steroid or hyaluronic acid...

What Are Back Spasms, and Can They Be Treated?
"Oh, my aching back!" Everyone has uttered these words at some point, in response to the sharp, sudden pain that comes with...

Arthritic Hands: What Works (and Doesn’t) to Ease the Pain?
Millions of people who live with the pain and stiffness of arthritis in their hands get steroid or hyaluronic acid...
Sciatica: What Is It, and How Can You Ease the Pain?
If you have had a sharp pain shooting down one leg, you may be experiencing a condition called sciatica. Here is what you...

Upper Back Pain: Causes and How to Treat It
If you suffer from upper back pain, it's time to reclaim your comfort and regain control of your daily life. Relief from...

Getting Rid of Neck Pain: 6 Ways to Feel Better
The phrase "pain in the neck" is a tongue-in-cheek way to describe annoying situations or people that test our patience,...
The Most Common Back Surgeries, Explained
Imagine a life where even the simplest movement becomes a painful endeavor. Back pain, a pervasive ailment affecting...

What Are Back Spasms, and Can They Be Treated?
"Oh, my aching back!" Everyone has uttered these words at some point, in response to the sharp, sudden pain that comes with...
When Arthritis Strikes, Keep Moving
Your achy joints may suggest that you take it easy. Don’t listen to them, experts say. If it hurts when you get up from a...

Have Arthritis? Take a Swing at Golf for Better Health
Could golfing be good medicine for arthritis? Yes, according to researchers who found that for people with osteoarthritis,...